Reinforced Composite COLTENE BRILLIANT Crios CAD/CAM Blocks

Patient Profiles
A 36-year-old female presented to clinic with fractured teeth and recurrent decay around existing amalgam restorations in the mandibular left quadrant. She admits to being negligent to dental procedures because of past traumatic experiences and anxiety.
The patient stated she is symptomatic to both pressure and temperature while functioning and denies any spontaneous or lingering pain. She complains of an intermittent odor, bad taste, and bleeding gums associated with the mandibular left quadrant.
The mandibular second molar (18) has a defective mesial-occlusal amalgam with a fracture along the mesial-lingual line angle and cusp. The first molar (19) has a defective mesial-occlusal-distal amalgam with extensive recurrent decay on both the mesial and distal proximal areas. The second premolar (20) has a defective distal-occlusal amalgam with extensive recurrent decay and a vertical fracture involving the mesial marginal ridge. The first premolar (21) has never been restored, but extensive distal decay has spread along the buccal cusp and the tooth has fractured (Fig.1).

Figure 1
The treatment plan for the patient’s mandibular left quadrant was designed for her current clinical condition and her anxious feelings towards dentistry. It was proposed to treat the mandibular left quadrant in a single appointment alleviating multiple visits attempting to mitigate the patient’s stress utilizing CAD/CAM (Primescan) technology. Teeth 19 and 21 were planned for full coverage crowns while teeth 18 and 20 were planned for three surface onlays (Table 1).
Tooth |
Surfaces |
Restoration |
|||
|---|---|---|---|---|---|
| 18 | MOL | Onlay | |||
| 19 | Full Coverage | Crown | |||
| 20 | MOD | Onlay | |||
| 21 | Full Coverage | Crown |
Table 1
The patient does not deny a history of clenching and bruxing her teeth. Clinical cases will often dictate to the clinician what dental materials will resist the mechanical forces applied while bruxing. Selecting the correct restorative dental material is essential to the long-term prognosis and the durability of the restoration. Dental ceramics have proven to be an exceptionally durable and esthetic material, but one of its weaknesses is its brittleness. These patients typically have lost their vertical dimension of occlusion (VDO) from enamel abrasion and present intraorally with vertically short clinical crown heights. This will limit the amount of occlusal reduction necessary to prepare a tooth for a ceramic restoration. The ceramic solution is to make the material harder, but increasing its strength also increases its brittleness.
Materials
The material selected was COLTENE’s BRILLIANT Crios reinforced composite blocks. The flexibility of Crios is determined by one of its unique physical properties (modulus of elasticity) and COLTENE has developed a material that closely resembles the elastic properties of dentin. Reinforced composites exhibit a comparable fracture resistance as ceramics but obtain this resistance with flexibility.
BRILLIANT Crios has several properties making it an ideal material selection for patients that exhibit parafunctional habits such as bruxism. Its 3-point and biaxial flexural strength allows it to withstand the habitual forces that will be applied without fracturing (Table 2).
Criteria |
Unit |
Method |
Value |
||||
|---|---|---|---|---|---|---|---|
| 3-point flexural strength | MPa | Internal | 198 | ||||
| Biaxial flexural strength | MPa | Internal | 262 | ||||
| Modulus of elasticity (Crios) | GPa | Internal | 10.3 | ||||
| Modulus of elasticity (Dentin) | GPa | Internal | 17.0 |
Table 2
The patient accepted the treatment plan, and a Chlorhexidine Gluconate (0.12%) oral rinse (Peridex) was prescribed to begin a forty-five second rinse twice a day one week prior to the appointment to control soft tissue inflammation and hemorrhaging.
After implementing and achieving a successful mandibular block the preparation of the teeth was performed for the appropriate restorations (Fig. 2).
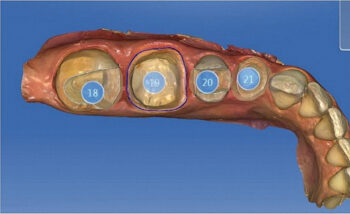
Figure 2
The restorations were designed using CEREC software 5.2.1 following the parameter guidelines for COLTENE BRILLIANT Crios CAD/CAM material (Fig. 3). The restorations were milled and the BRILLIANT Crios material was treated according to protocols prior to bonding.
In contrast to ceramic materials, CAD/CAM composites must always be luted adhesively. This implies an adhesive bond between composite restoration and luting material as well as between luting material and tooth substance. Depending on the indication, light-curing composites or adhesive resin cement are suitable.

Figure 4
Conclusion
After manufacturing the restoration, the intaglio surface (internal) to be bonded is sandblasted to increase the surface area and to create mechanical retention. Corundum (aluminum oxide) is used as the blasting medium. The effect of the sandblasting procedure is comparable to pre-treatment through sandblasting for zirconia or etching with hydrofluoric acid for silicate ceramics. It is critical to remember you cannot acid etch CAD/CAM composites. The sandblasted surface now contains particles of dental glass and polymerized resin matrix. The ratio is approximately 1:1.
To ensure a permanent bond it is therefore important to achieve adhesion to both the glass fillers as well as the resin matrix. Carboxylic acid groups or MDP (10-Methacryloyloxydecyl dihydrogen phosphate) create a strong bond to the fillers and combined with dysfunctional monomers (ONE COAT 7 UNIVERSAL) a strong bond to the resin matrix is achieved (Fig. 4).
Written by Samuel L. Corey, DDS
Permission to publish provided by COLTENE.
![]()
Published in TIPS – March/April 2021
Category: Merchandise
Back to Articles